|
Home > Patient Information > ERCP
ERCP
What is an ERCP?
Endoscopic Retrograde Cholangio-Pancreatography
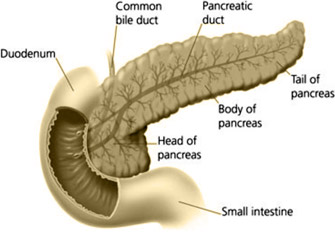
ERCP is an endoscopic procedure performed under x-ray guidance, for the diagnosis and treatment of conditions affecting the biliary system and pancreas.
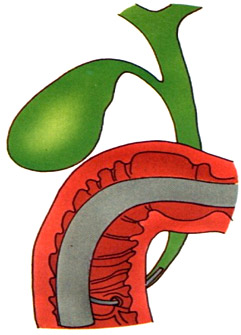
The biliary system includes the bile ducts, which are the tubes draining the liver, and the gallbladder.
You will have sedation or an anaesthetic for the procedure, and will not be awake or aware of anything.
Problems with the bile ducts or pancreas may present as jaundice or pain in the abdomen. Blood tests may show abnormalities of the liver or pancreas. Imaging tests such as ultrasound, CT scan, and MRI may be done. Disorders affecting the pancreas and biliary system, can then be managed with ERCP.
ERCP is helpful when there is a blockage of the bile ducts by gallstones or tumours, which cause obstruction or narrowing (stricture) of the ducts. Similarly, blockage of the pancreatic duct by stones, tumours, or stricture can also be managed with ERCP, along with helping to sort out the cause of pancreatitis (inflammation of the pancreas). ERCP is used to diagnose and treat a leak of bile after liver trauma or gall bladder surgery.
As part of the ERCP, you may have:
- a sphincterotomy, which is a small cut in the muscle at the point where the bile and pancreatic duct insert into the duodenum (ampulla). This is to help remove stones or insert a drainage tube called a stent.
- Stent/s are inserted inside the bile duct or the pancreatic duct. For example: when all the stones cannot be removed or when there is blockage or leak to overcome. Also to protect against pancreatitis a temporary pancreatic stent may be inserted. A bile duct stent may be inserted for weeks to months at a time if needed. A plastic stent will need to be removed at some stage (usually after a few weeks) or it may block and cause infection. Metal stents are usually placed permanently.
Before the Procedure,
- We need to know about all the medications you are taking, in particular if you take aspirin or other blood thinners such as clopidogrel (plavix, iscover), or warfarin.
- Keep taking all your usual medications unless otherwise instructed. Diabetics need special instructions.
- Do you have any allergies to antibiotics, pain medications or other drugs?
- You need to fast (nothing by mouth) for 6 hours (solids and dairy) before the ERCP, however clear fluids (water, clear apple juice, Gatorade) can be taken up 2 hours before the procedure.
What are the Possible Complications from an ERCP?
Depending on the individual and the type of procedures performed, ERCP carries a five to ten percent risk of complications, which are rarely ever severe.
Minor complications
- Mild discomfort inside the abdomen due to retained air in the bowel, may occur in the first hour.
- A sore throat from the endoscope or anaesthetic tube may last a couple of days.
- Loose teeth, crowns and bridgework may rarely be dislodged.
- Irritation, bruising or a lump where a drip was inserted for intravenous medications.
- Reactions may occur to any of the medications used during ERCP. Usually, these are minor.
- Pancreatitis occurs in less than 5% of ERCPs (1 in 20 cases). This means mild inflammation of the pancreas, which causes pain in the abdomen due to swelling in the pancreas. In 90% of cases pancreatitis settles within one or two days, with a drip and pain relief.
Major complications
- More severe inflammation of the pancreas is a rare complication and may require longer hospital care, intensive care, and even surgery or further procedures to drain intraabdominal infection and fluid collections (less than 1 in 200 ERCPs).
- Although it is very rare, severe pancreatitis can be fatal (less than 1 in 2000 ERCPs)
- If sphincterotomy is performed, bleeding may occur. Bleeding usually stops quickly by itself, but occasionally, blood transfusion may be required. Rarely, the bleeding has to be controlled by repeat endoscopy, a special x-ray procedure, or surgery.
- A hole or perforation of the bowel wall or bile duct is a rare problem that can occur with ERCP, due to the endoscope or during sphincterotomy. Surgery may be needed to repair the perforation.
- Infection can occur, especially if the bile duct is blocked and bile cannot drain. Treatment for infection requires antibiotics and restoring drainage. Antibiotics may be given in some patients before ERCP, to prevent this complication.
- Aspiration of stomach fluid into the lung can cause pneumonia in very frail or sick patients.
What happens after the ERCP?
- Most outpatients will be discharged on the same day. You will need someone to drive you, since you’re likely to be sleepy from the sedative you received. Avoid operating machinery, drinking alcohol for 24 hours.
- Your doctor will tell you when you can take fluids and meals. Usually, it is within a few hours of the procedure finishing.
- When you get home, if you notice bleeding from your rectum or black, tarry stools, OR vomiting, OR severe abdominal pain, OR weakness OR dizziness, OR fever over 37.5 degrees, seek medical advice. These problems are not common, but if you become unwell, you will need to call the hospital to speak to a doctor or present to the Emergency Department.
If you have any questions about the procedure or are unsure about what you need to do beforehand or what will happen afterwards please call my rooms on 5539 1240. Be sure to discuss any specific concerns you may have about the procedure with your doctor.
|
|